9 Min Read
9 Min Read
Pregnancy is a journey marked by excitement, anticipation, and memorable milestones. Yet for some women, worries about the health of their pregnancy and the possibility of carrying their baby safely to term can become a major source of anxiety and uncertainty.
One condition that may increase the risk of pregnancy loss or premature birth is cervical insufficiency (the historical terminology was "cervical incompetence," which has shifted to "cervical insufficiency," which is a more clinical and neutral term). In this condition, the cervix begins to shorten or open too early without contractions. In carefully selected cases, a cervical cerclage procedure can help provide additional support to the cervix and improve the chances of continuing the pregnancy for longer.
While hearing that you may need a surgical intervention during pregnancy can feel unsettling, understanding why it is recommended and what it involves often brings reassurance. In this blog, a top obstetrician and gynaecologist in Hebbal, Bangalore, explains what cervical cerclage is, when it may be advised, the different techniques available, including laparoscopic abdominal cerclage, the benefits and risks involved, and what you can expect before and after the procedure.
Synopsis
- Understanding Cervical Insufficiency
- What Is Cervical Cerclage?
- When Is Cervical Cerclage Recommended?
- Different Methods of Cervical Cerclage
- Laparoscopic Abdominal Cerclage: An Advanced Approach
- Benefits of the Cervical Cerclage Procedure
- Comparing Different Cerclage Approaches
- Recovery and What to Expect Afterwards
- Possible Risks and Complications
- Conclusion
Understanding Cervical Insufficiency
The cervix plays a vital role during pregnancy by remaining closed and firm until labour begins. In some women, however, the cervix may weaken and start opening too early, often during the second trimester.
This condition is known as cervical insufficiency. It can occur without pain, contractions, or obvious warning signs, making regular prenatal monitoring especially important for women with a history of pregnancy complications.
Factors that may increase the risk include:
-
Previous second-trimester pregnancy losses
-
Prior cervical surgery, such as a cone biopsy or extensive cervical procedures
-
Congenital abnormalities affecting the cervix or uterus
-
Previous traumatic cervical injury during childbirth
-
A history of unsuccessful cerclage in an earlier pregnancy
What Is Cervical Cerclage?
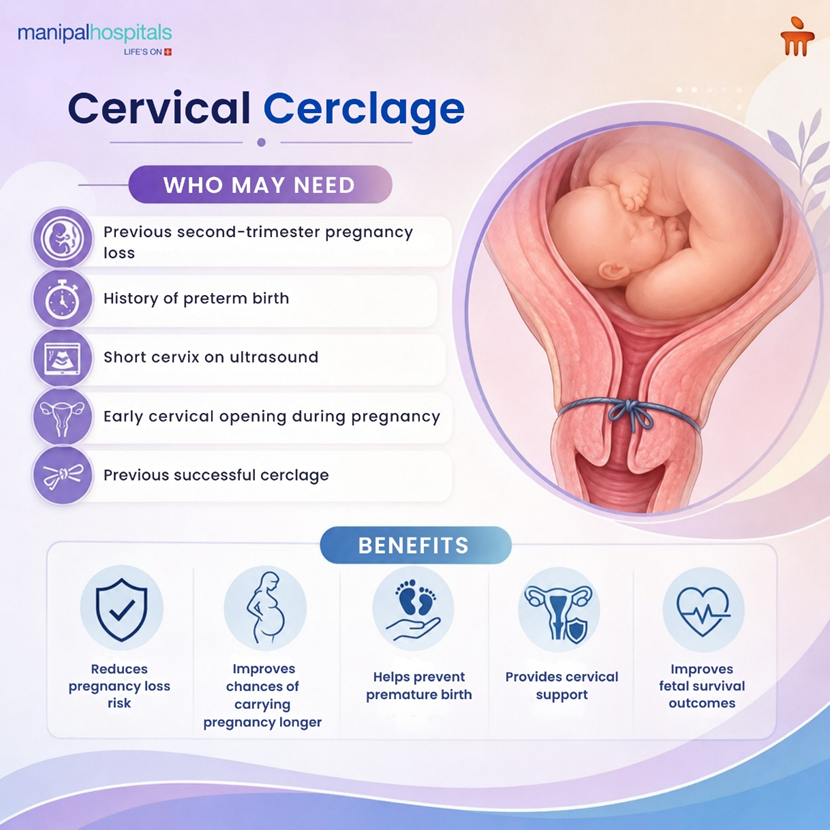
Understanding what cervical cerclage is helps many women feel more confident when discussing treatment options with their obstetrician. The procedure involves placing a strong stitch around the cervix to help keep it closed during pregnancy.
The stitch acts as mechanical support, reducing the likelihood of premature cervical opening. It is generally performed between 12 and 24 weeks of pregnancy, depending on the clinical situation and the reason for intervention. Most women undergo the procedure under regional or general anaesthesia and return home within a short period after observation.
When Is Cervical Cerclage Recommended?
The decision to perform a cerclage is based on a combination of medical history, ultrasound findings, and current pregnancy assessment. Understanding common cervical cerclage indications can help you appreciate why your doctor may recommend the procedure.
A cerclage may be advised when:
-
There is a history of one or more painless second-trimester pregnancy losses
-
Previous spontaneous preterm births were associated with cervical shortening
-
Ultrasound shows a significantly shortened cervix during pregnancy
-
The cervix has already begun to dilate before viability without labour
-
A previous pregnancy benefited from cerclage placement
Not every woman with a short cervix requires a stitch. Your specialist will consider multiple factors before recommending treatment.
Specific Clinical Situations Where Cerclage May Be Recommended:
-
History-Indicated Cerclage: Women with a history of one or more spontaneous second-trimester pregnancy losses or spontaneous preterm births related to cervical insufficiency may be advised to undergo cerclage placement in a subsequent pregnancy.
-
Ultrasound-Indicated Cerclage: In women with a singleton pregnancy and a history of spontaneous preterm birth before 34 weeks of gestation or a mid-trimester pregnancy loss, an ultrasound-indicated cerclage may be recommended if transvaginal ultrasound demonstrates a cervical length of less than 25 mm before 24 weeks of gestation.
-
Women Without a Prior Preterm Birth: For women with a singleton pregnancy, no prior spontaneous preterm birth, and otherwise normal obstetric risk factors, cervical cerclage is generally not recommended routinely. However, it may be considered if the cervix shortens to less than 10 mm before 24 weeks of gestation despite progesterone therapy, following specialist assessment.
-
Rescue (Emergency) Cerclage: A rescue cerclage, also known as an emergency cerclage or physical examination-indicated cerclage, is performed when the cervix has already begun to dilate during pregnancy but labour has not started.
-
This procedure is usually carried out during the second trimester (approximately 14–24 weeks of gestation) to help prevent a late miscarriage or extremely premature birth.
Rescue cerclage may be considered:
-
When the cervix is already opening on examination
-
Fetal membranes are visible or bulging through the cervical opening
-
There is no evidence of active labour
-
There are no signs of intrauterine infection
Although technically more challenging than planned cerclage procedures, rescue cerclage may help prolong pregnancy and improve neonatal outcomes in carefully selected patients.
Different Methods of Cervical Cerclage
Several techniques are available, and the most appropriate approach depends on your individual circumstances. Understanding the different types of cervical cerclage can make discussions with your healthcare team easier.
-
McDonald Cerclage: This procedure is the most commonly performed method worldwide. A purse-string stitch is placed around the cervix through the vagina and tightened to provide support. It is technically straightforward, highly effective in suitable candidates, and typically removed in the near term before labour begins.
-
Shirodkar Cerclage: This technique places the stitch slightly higher within the cervix. It may be chosen when additional support is required or when anatomical considerations make placement more challenging. The procedure is more technically demanding but can offer advantages in selected cases.
-
Transabdominal Cerclage: Some women are not suitable candidates for a vaginal cerclage, particularly if they have significant cervical shortening, previous failed vaginal cerclage, or cervical anatomical abnormalities. In these situations, a transabdominal approach may be considered.
Laparoscopic Abdominal Cerclage: An Advanced Approach
Advances in minimally invasive surgery have transformed how certain high-risk pregnancies are managed. Laparoscopic abdominal cerclage offers an alternative for women who may not benefit from conventional vaginal techniques.
Using small abdominal incisions and specialised instruments, the surgeon places a supportive band at the upper part of the cervix. Compared with traditional open surgery, laparoscopy generally results in:
-
Smaller scars
-
Less postoperative discomfort
-
Shorter hospital stays
-
Faster recovery
-
Reduced blood loss
The stitch is usually left in place for future pregnancies, meaning delivery is typically performed by cesarean section.
Benefits of the Cervical Cerclage Procedure
When recommended for the right reasons, a cervical cerclage procedure can play an important role in improving pregnancy outcomes.
Potential benefits include:
-
Reduced risk of second-trimester pregnancy loss
-
Increased likelihood of reaching later gestational milestones
-
Improved chances of fetal survival
-
Greater cervical stability throughout pregnancy
-
Psychological reassurance for women with previous pregnancy losses
While no intervention can guarantee a full-term delivery, carefully selected women often experience meaningful benefits from treatment.
Comparing Different Cerclage Approaches
Choosing the right technique depends on several clinical factors. The table below highlights the key differences between the commonly used approaches.
|
Feature |
McDonald Cerclage |
Shirodkar Cerclage |
Laparoscopic Abdominal Cerclage |
|
Surgical access |
Vaginal |
Vaginal |
Abdominal (laparoscopic) |
|
Technical complexity |
Lower |
Moderate |
Higher |
|
Typical operating time |
Shorter |
Moderate |
Longer |
|
Suitability for severe cervical shortening |
Limited |
Moderate |
Often preferred |
|
Future pregnancies without repeat procedure |
Usually not |
Usually not |
Often, yes |
|
Requirement for caesarean delivery |
Not always |
Not always |
Yes |
|
Stitch removal before delivery |
Usually required |
Usually required |
Usually remains in place |
Recovery and What to Expect Afterwards
Recovery following cervical cerclage surgery is generally straightforward. Mild cramping, light spotting, and pelvic discomfort may occur during the first few days. Most women can resume many normal daily activities after their doctor's approval. Follow-up appointments are important because they allow monitoring of cervical length and assessment of overall pregnancy progress.
Your healthcare provider may advise you to contact the hospital if you experience:
-
Persistent contractions
-
Leakage of fluid
-
Fever
Following up on your recommendations helps ensure that any concerns are addressed promptly.
Possible Risks and Complications
Although generally safe, every surgical procedure carries some degree of risk. Understanding potential cervical cerclage complications allows you to make informed decisions.
Possible complications include:
-
Infection involving the membranes or uterus
-
Bleeding during or after the procedure
-
Premature rupture of membranes
-
Cervical laceration
-
Anaesthesia-related complications
-
Uterine contractions triggered by the procedure
Fortunately, serious complications remain uncommon when performed by experienced specialists in appropriately selected patients.
Conclusion
A cervical cerclage procedure can be a valuable option for women at risk of pregnancy loss or premature birth due to cervical insufficiency. With careful assessment, timely intervention, and ongoing monitoring, many women are able to continue their pregnancies safely and achieve better outcomes. Understanding the available approaches, including vaginal techniques and advanced laparoscopic abdominal cerclage, can help you feel more informed and confident about your care journey.
If you are exploring options for cervical cerclage treatment in Hebbal, Bangalore, seeking evaluation from an experienced maternal-fetal medicine specialist is essential. Manipal Hospital Hebbal offers comprehensive high-risk pregnancy care, advanced surgical expertise, and personalised support throughout your pregnancy.
FAQ's
Yes. In certain high-risk situations, particularly when a woman has experienced repeated pregnancy losses related to severe cervical weakness, an abdominal cerclage may be placed before conception. This approach allows the stitch to be positioned under optimal surgical conditions before pregnancy begins.
No. Cerclage itself does not reduce fertility or make conception more difficult. Women who require a transabdominal cerclage can still become pregnant naturally unless another unrelated fertility issue is present.
Travel recommendations depend on your pregnancy risk profile, gestational age, and overall health. Some women can travel safely after recovery, while others may be advised to remain close to specialised obstetric care. Individual guidance from your doctor is important.
Yes. With a structured treatment approach involving explanation, physiotherapy, and psychological support, many people with functional neurological disorder experience substantial improvement or complete resolution of symptoms.
Not necessarily. The purpose of the stitch is primarily to provide structural support and reduce further cervical opening. Ultrasound measurements may remain stable, shorten slowly, or occasionally continue changing despite successful placement.
Occasional forgetfulness is normal at any age. However, persistent memory loss that interferes with daily activities, especially if it progresses over months and is accompanied by changes in personality or reasoning, warrants evaluation regardless of age.
Yes. Although many women diagnosed with cervical insufficiency have a history of pregnancy loss or preterm birth, some experience the condition for the first time during an otherwise uncomplicated pregnancy. This is why routine antenatal scans remain an important part of prenatal care.
Share this article on: