12 Min Read
12 Min Read
Pelvic organ prolapse (POP) is a common problem in older women, particularly after the menopause. Over time, the supporting muscles and connective tissues of the pelvic floor may weaken, which can allow such organs as the uterus, bladder, rectum, or small bowel to descend into or beyond the vaginal canal. Some women have only mild symptoms, but some develop significant discomfort that affects mobility, bladder and bowel function, activities of daily living, and quality of life.
As life expectancy increases, more women are presenting for treatment of pelvic floor disorders in their seventies and beyond. But many also suffer from age-related medical conditions like heart disease, diabetes, or hypertension, which complicates treatment decisions.
Many people think that if you're older or have multiple medical problems, surgery is out of the question. In this blog, an experienced obstetrician and gynaecologist from Hebbal, Bengaluru, takes you through a real clinical case to show how treatment decisions should not be based on age alone, but on a thorough evaluation of the patient’s overall health, functional status, symptoms, goals, and quality-of-life expectations.
This case emphasizes the importance of multidisciplinary planning and individualized decision-making in a 73-year-old woman with significant cardiovascular risk factors to safely undergo definitive surgical treatment for advanced pelvic organ prolapse.
Synopsis
Understanding Pelvic Organ Prolapse in Older Women
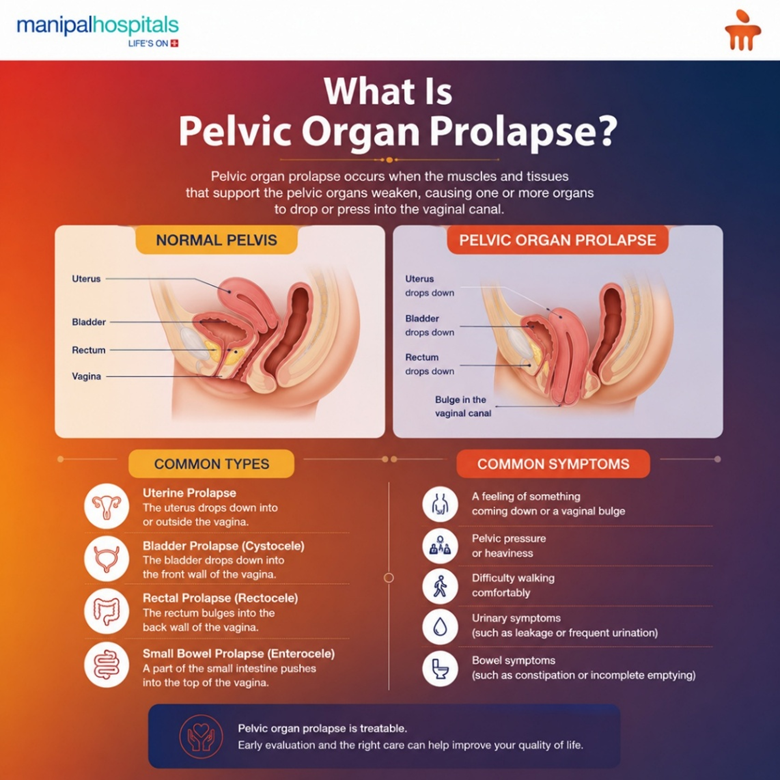
Pelvic organ prolapse is a weakening or stretching of the pelvic floor structures that support the pelvic organs. Prolapse can present as the following, depending on the structures involved:
-
Uterine prolapse (descent of the uterus)
-
Cystocele (bladder prolapse)
-
Rectocele (prolapse of the rectum into the vaginal wall)
-
Enterocele (herniation of small bowel into vaginal space)
Women may experience:
-
A sensation of something “coming down” from the vagina
-
Pelvic pressure or heaviness
-
Difficulty walking comfortably
-
Urinary symptoms
-
Bowel symptoms
-
Reduced quality of life
While conservative options such as pelvic floor exercises and pessary use can be effective for many women, some patients ultimately require surgical correction.
The Case
A 73-year-old woman presented with Grade 3 uterovaginal (UV) prolapse associated with Grade 3 cystocele, Grade 3 rectocele, and enterocele, which was beginning to significantly impact her daily life and comfort. The condition had progressed to the point that the uterus and nearby pelvic organs, such as the bladder and bowel, had slipped down from their normal positions because the pelvic floor muscles and supporting tissues had become weaker. She had symptoms that persisted and affected her quality of life and made daily activities progressively uncomfortable.
This case was particularly challenging due to the patient’s medical history. She was on long-term blood-thinning medications, which were discontinued one week prior to surgery as part of the preoperative planning process. She also had a history of diabetes, hypertension, and coronary artery disease for which she had undergone coronary angioplasty with placement of 4–5 stents approximately 1.5 years earlier. Her age and multiple medical problems made the decision to proceed with surgery a difficult one. But she was active, independent, and very motivated to find a definitive solution after conservative treatment with a pessary failed to provide adequate relief.
The Clinical Dilemma: Prolapse and Cardiac Risk
The prolapse itself was severe and amenable to surgical correction. But the fact that there was significant cardiovascular disease made it even more difficult. Multiple other factors required careful consideration:
-
Ageing
-
Prior coronary angioplasty with placement of 4–5 coronary stents (approximately 1.5 years earlier)
-
Continuous antiplatelet therapy
-
Diabetes mellitus
-
Potential for perioperative cardiovascular risk
Management Options Considered
As is common in women presenting with advanced prolapse, multiple treatment pathways were evaluated.
-
Pessary management continued: A ring pessary had previously been fitted as a conservative treatment option. Pessaries are very effective in some patients, but this patient was unable to tolerate the device and remained symptomatic.
-
Obliterative Procedures: In elderly women who do not desire vaginal function and want relief of symptoms with a shorter operation, procedures such as colpocleisis may be considered.
-
Reconstructive Vaginal Surgery: Definitive surgical repair with vaginal surgery was a possibility to correct the prolapse with restoration of pelvic support and improvement in long-term quality of life.
Ultimately, it was a matter of the risk of surgery vs. symptoms.
Why Was Surgery Still Considered?
The patient was 73 years old and had a history of heart disease, but age was not viewed as a barrier to treatment. Her symptoms were significantly affecting her quality of life, conservative management had failed, and she was still active and independent and keen to pursue a definitive solution. They didn’t just consider her age and medical conditions but also her overall health, functional status, and ability to safely undergo surgery.
Why is multidisciplinary planning Important?
Given her significant cardiac history, careful multidisciplinary planning was essential. The patient was thoroughly assessed by gynaecologists, cardiologists and anaesthetists to evaluate her cardiac status, optimise her diabetes and blood pressure, review her antiplatelet medications, and minimise surgical risk.
Notably, the patient's earlier coronary angioplasty had been performed by Dr. Kumar Kenchappa, the top interventional cardiologist in Manipal Hospital Hebbal, who played a significant role in the multidisciplinary team approach. His expertise and guidance in optimising the patient's cardiac condition were instrumental in making definitive surgical treatment possible. This collaborative planning helped ensure that the team could perform the procedure as safely as possible.
Procedure(s) Performed:
The patient was prepared and underwent vaginal hysterectomy and repair of the prolapse and re-establishment of support of the organs after preoperative optimisation and medical clearance. The surgery was safely completed with minimal blood loss, and regional anaesthesia techniques were used to support postoperative pain control and recovery.
Why was vaginal surgery chosen?
In selected patients with advanced pelvic organ prolapse, vaginal surgery has several advantages including:
-
Prolapse: The vaginal approach allows direct visualization of the prolapsed structures and avoids abdominal incisions.
-
Lower Surgical Morbidity: Vaginal surgery is generally less stressful surgically than more extensive abdominal procedures.
-
Faster Recovery and Mobilisation: Early ambulation is especially important in elderly patients to decrease postoperative complications.
-
Effective Anatomical Correction: Vaginal repair can address many pelvic floor defects at the same time.
This was a balanced approach for this patient, which treated the prolapse and decreased the surgical burden at the same time.
Outcome and Rehabilitation
The operation was done successfully with minimal blood loss and no major complications. The patient’s recovery was uneventful, and she was able to mobilise early and be ambulant within 48 hrs. Despite her age and underlying cardiac condition, she received the definitive treatment she sought and was discharged shortly thereafter.
Key Takeaways
-
Women should not be denied prolapse surgery on the basis of advanced age alone.
-
Management of pelvic organ prolapse must be individualised.
-
Conservative options remain important, but not appropriate for every patient.
-
Previous coronary angioplasty with coronary stenting is not an absolute contraindication to surgery when appropriate cardiac evaluation and optimisation are undertaken.
-
The multidisciplinary cooperation of gynaecologists, cardiologists, and anesthesiologists may lead to better safety.
-
Preoperative optimisation is important to reduce perioperative risk.
The goal is not just to perform surgery but to improve the quality of life while keeping patients safe.
Conclusion
Pelvic organ prolapse can have a significant impact on comfort, mobility, independence, and overall quality of life, particularly in older women. Although age and medical comorbidities may influence surgical complexity, they should not preclude patients from definitive treatment. Successful outcomes are achievable with careful assessment, multidisciplinary planning, and patient-centered decision-making, even in high-risk individuals.
If you or someone you love is looking for pelvic organ prolapse treatment in Hebbal, Bangalore, book an appointment with our top gynaecology experts at Manipal Hospital Hebbal, recognised for its Obstetrics and Gynaecology speciality hospital near Hebbal, to discuss the best-suited treatment options for your condition and lifestyle goals.
FAQ's
Yes. Many women do well with pelvic floor exercises, lifestyle changes, and pessaries. The best option depends on the severity of symptoms, the stage of prolapse, and individual preferences.
It is not just age that determines suitability for surgery. Many older women can be safely operated on following appropriate assessment and optimisation.
A pessary is a removable medical device that is inserted into the vagina to support the prolapsed pelvic organs and relieve symptoms without surgery.
Most women with heart disease can have surgery safely after thorough evaluation by cardiologists, anesthesiologists, and surgeons. The choice depends on individual general health and cardiovascular status.
Recovery depends on the procedure and the patient’s overall health. Early mobilisation and gradual return to normal activities over several weeks is encouraged in most patients.
Share this article on: