9 Min Read
9 Min Read
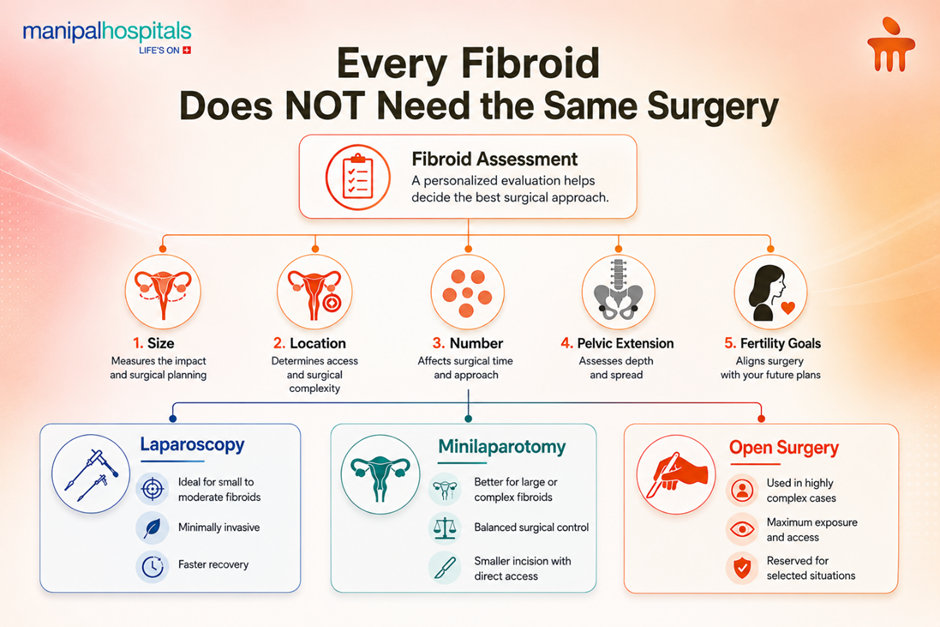
Uterine fibroids are common, but the way they affect each woman can be very different. Some fibroids stay small and never cause major trouble. Others grow quietly over time and begin to press on nearby organs, disturb daily life, and complicate treatment. When fibroids become huge or are located in difficult areas of the pelvis, the treatment plan needs to be chosen carefully, not just to remove the fibroid, but also to protect the uterus, surrounding structures, and long-term recovery.
While laparoscopy is widely preferred for many fibroid cases, it is not always the most suitable option in technically demanding scenarios. In such situations, selecting the right surgical approach becomes crucial. Options may include laparoscopy, open surgery, or hybrid techniques such as minilaparotomy, each with its advantages depending on the complexity of the case.
In this blog, an experienced obstetrician and gynaecologist in Hebbal, Bengaluru, walks you through a real clinical case to highlight how minilaparotomy myomectomy can offer a balanced, effective alternative—combining controlled access with minimally invasive principles.
Synopsis
The Case Study
A 37-year-old woman was diagnosed with multiple large fibroids. Two major fibroids were identified.
-
A 15 cm fundal fibroid
-
A 20 cm fibroid arising near the isthmus, extending retroperitoneally over the rectum and along the lateral pelvic wall
This second fibroid mimicked a pseudo-broad ligament / retroperitoneal mass, significantly distorting pelvic anatomy and extending into the rectovaginal space.
Such anatomy presents three key surgical concerns:
-
Difficulty in identifying normal tissue planes
-
Increased risk to adjacent structures (rectum, bladder, vessels)
-
Limited feasibility of standard minimally invasive techniques
Surgical Planning: Why Approach Matters
In large and complex fibroids, the goal is not just removal; it is safe, controlled removal with preservation of surrounding structures.
Key considerations in this case included:
-
Size and deep pelvic extension
-
Distorted anatomy
-
Need for intact removal
-
Minimising blood loss
-
Avoiding injury to bowel and adjacent organs
Rather than defaulting to laparoscopy or open surgery, a tailored approach was chosen.
Procedure Performed
The operation was performed through a minilaparotomy, using a 4–6 cm incision, and the myomectomy for large fibroids was completed without morcellation.
Key intraoperative details:
-
200 mL normal saline with vasopressin infiltration was used to minimise bleeding
-
Fibroids were removed intact (no morcellation)
-
Blood loss was near nil
-
The uterus and adnexa were preserved
-
Rectal integrity was carefully assessed and maintained
-
Dissection planes were largely avascular, allowing controlled removal
Why Not Laparoscopy in This Case?
Laparoscopy is highly effective in many fibroid surgeries. However, in this scenario, it presented limitations:
-
Difficulty handling very large fibroids (15–20 cm)
-
Challenging access due to deep pelvic extension
-
Likely requirement of morcellation for specimen removal
-
Reduced tactile feedback in distorted anatomy
While laparoscopy offers faster recovery in suitable cases, it may compromise control and safety in complex anatomical situations.
Why Was Minilaparotomy Preferred?
Minilaparotomy is often described as a bridge between open surgery and laparoscopy. It provides a practical middle path, retaining advantages of both open and minimally invasive techniques.
Key advantages in this case
-
Better Surgical Control: Direct access allowed precise dissection around the rectum and pelvic structures.
-
Tactile Feedback: The ability to feel tissue planes is particularly valuable in distorted anatomy.
-
Intact Fibroid Removal: Avoided morcellation and associated concerns.
-
Minimal Blood Loss: Use of vasopressin and avascular planes ensured excellent haemostasis.
-
Smaller Incision, Faster Recovery: Reduced surgical trauma compared to conventional open surgery.
Minilaparotomy vs Laparoscopy: Practical Comparison
|
Surgical Aspect |
Laparoscopy |
Minilaparotomy |
|
Approach |
Fully minimally invasive |
Hybrid approach |
|
Suitability |
Ideal for small to moderate fibroids |
Better for large/complex fibroids |
|
Access |
Limited in deep or distorted anatomy |
Direct and controlled |
|
Tactile feedback |
Absent |
Present |
|
Morcellation |
Often required |
Usually avoided |
|
Incision size |
Very small |
Small (4–6 cm) |
|
Recovery |
Fast |
Comparable, slightly longer than laparoscopy but shorter than open surgery |
|
Safety in complex cases |
Can be challenging |
More controlled |
The Role of Morcellation
Morcellation is often used in laparoscopic surgery to remove large fibroids through small incisions. However, it has limitations:
-
Fragmentation of tissue
-
Risk (though rare) of spreading undetected malignancy
-
Reduced pathological clarity
In this case, intact removal through minilaparotomy eliminated these concerns, offering both safety and completeness.
Clinical Significance of Blood Loss Control
A critical highlight of this surgery was near nil blood loss, achieved through:
-
Vasopressin infiltration (200 mL NS with vasopressin)
-
Careful identification of avascular planes
-
Controlled dissection
This significantly improves:
-
Surgical safety
-
Postoperative recovery
-
Overall patient outcomes
Key Takeaways
-
Not all fibroids should be approached the same way; size and location matter
-
Large, deeply located fibroids require individualised surgical planning
-
Laparoscopy is not always ideal in complex anatomy
-
Minilaparotomy offers a balanced approach, control + minimal invasiveness
-
Intact removal without morcellation can be advantageous in selected cases
-
Proper technique can result in near-zero blood loss and excellent outcomes
-
The goal is not the newest technique, but the safest and most appropriate one
Conclusion
Fibroids are common, but large and complex fibroids require careful surgical judgement. This case shows how a well-planned minilaparotomy myomectomy remains highly relevant in modern obstetrics and gynaecology care in Hebbal, Bangalore, especially for large and complex fibroids. By combining direct surgical control, smaller incisions, tactile precision, and avoidance of morcellation,
Experienced obstetrics and gynaecology doctors near Hebbal, Bangalore, offer a safe, efficient, and patient-centric solution when laparoscopy is not ideal.
Ultimately, the success of fibroid surgery lies not in choosing a single technique but in choosing the right technique for the right patient.
FAQ's
Yes, in many cases, large fibroids can be removed through a procedure called "myomectomy," where only the fibroids are taken out, and the uterus is preserved. The decision depends on factors such as the size, number, and location of the fibroids, as well as your symptoms and future fertility plans.
It is less invasive than open surgery and involves a small incision, offering a balance between safety and recovery.
Morcellation is a technique used to break large fibroids into smaller pieces so they can be removed through small incisions, usually during laparoscopic surgery. While it helps maintain a minimally invasive approach, it is sometimes avoided because of the risk of spreading undetected abnormal or cancerous tissue, such as uterine sarcoma, within the abdomen.
Recovery after a minilaparotomy is usually faster than traditional open surgery but may take slightly longer than laparoscopy. Most patients begin walking within a day and gradually return to normal activities over 2–4 weeks, depending on their overall health and the complexity of the surgery.
Techniques like vasopressin infiltration and careful dissection help minimise bleeding significantly.
Share this article on: