Cs Narayanan VSM | Best Neurologist in Delhi | Manipal Hospitals")
 6 Min Read
6 Min Read
If you've ever experienced sudden, intense, electric shock-like pain at the back of your head or neck, extending towards your scalp, you might be familiar with the debilitating symptoms of occipital neuralgia. This condition, often mistaken for other types of headaches, arises from irritation or injury to the occipital nerves. Understanding its origins and available treatments is crucial for finding relief and improving quality of life. Our neurologists in Delhi are at the forefront of diagnosing and treating complex neurological conditions like occipital neuralgia, employing advanced techniques and compassionate care.
Synopsis
- Understanding Occipital Neuralgia
- The Anatomy of Occipital Nerves
- Unravelling the Causes of Occipital Neuralgia
- Recognising Occipital Neuralgia Symptoms
- Diagnosing Occipital Neuralgia
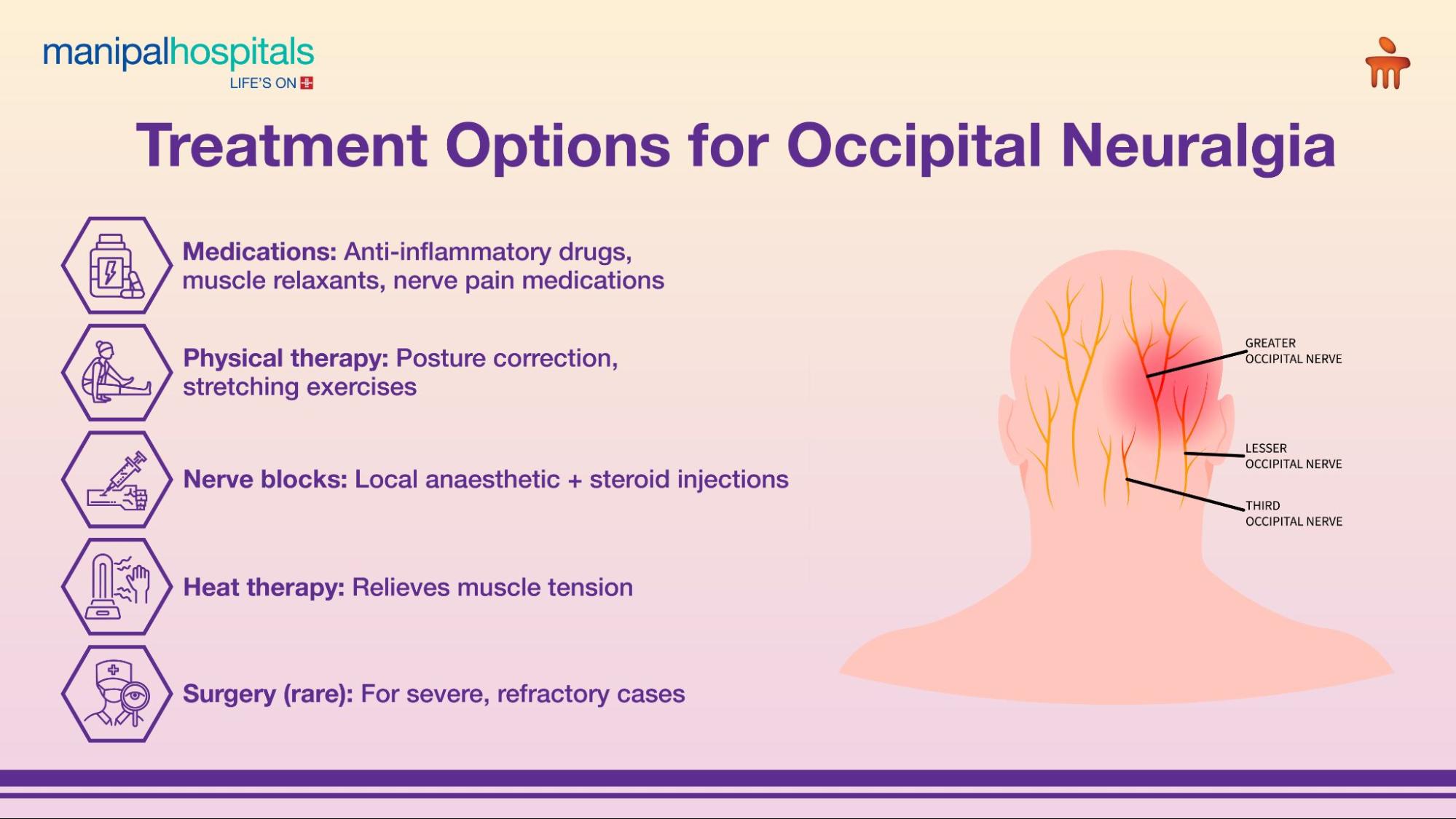
- Occipital Neuralgia Treatment Options The goal of occipital neuralgia treatment is to alleviate pain, reduce inflammation, and address any underlying causes. Treatment approaches range from conservative therapies to advanced interventions, with a high success rate in pain reduction for many patients, often exceeding 70-80% with combined therapies. Conservative Treatments for Occipital Neuralgia Relief: Heat and Cold Therapy: Applying heat packs to the neck and cold packs to the scalp can help reduce muscle tension and inflammation, offering temporary relief. Massage and Physical Therapy: Specific massage techniques and physical therapy exercises can help release tight neck muscles, improve posture, and alleviate nerve compression. This can significantly reduce pain in up to 60% of patients. Over-the-Counter Pain Relievers: Non-steroidal anti-inflammatory drugs (NSAIDs) can help manage mild to moderate pain and inflammation. Prescription Medications: Your doctor may prescribe muscle relaxants to ease muscle spasms, anticonvulsants for nerve pain, or antidepressants that also have pain-relieving properties for more persistent symptoms. Nerve Blocks: Therapeutic occipital nerve blocks, similar to diagnostic ones, involve injecting a local anaesthetic, sometimes combined with a corticosteroid, directly around the affected nerve. These can provide several weeks to months of occipital neuralgia relief and are effective for approximately 75% of patients. Botulinum Toxin Injections: For chronic, refractory cases, injections of botulinum toxin into the muscles around the occipital nerves can help relax them, reducing compression and providing sustained pain relief for up to three months in about 65% of cases.
- Advanced Interventions
- Living with Occipital Neuralgia: Prevention and Management
Understanding Occipital Neuralgia
What is Occipital Neuralgia?
Occipital neuralgia is a type of headache characterised by chronic pain in the upper neck, back of the head, and behind the ears. It typically occurs when the occipital nerves – specifically the greater and lesser occipital nerves that run from the spinal cord through the muscles at the back of the head to the scalp – are damaged, inflamed, or compressed. This nerve pain often manifests as a sharp, piercing, or throbbing sensation, sometimes accompanied by tenderness on the scalp. Unlike migraines, occipital neuralgia rarely presents with auras but can be equally disruptive, impacting daily activities and sleep patterns.
The Anatomy of Occipital Nerves
To fully grasp occipital neuralgia, it's helpful to understand the role of the occipital nerves. These sensory nerves transmit information from the scalp to the brain. The greater occipital nerve is the largest and most commonly affected, originating from the C2 and C3 spinal nerves and supplying sensation to the back of the head up to the crown. The lesser occipital nerve, also arising from C2/C3, supplies the skin behind the ear and the side of the head. When these nerves are irritated, compressed, or injured, they can send abnormal pain signals, leading to the distinctive occipital nerve pain associated with the condition.
Unravelling the Causes of Occipital Neuralgia
The causes of occipital neuralgia can vary widely, ranging from identifiable physical conditions to idiopathic origins. Pinpointing the exact cause is a critical step in developing an effective occipital neuralgia treatment plan.
Primary Causes (Idiopathic)
In some cases, occipital neuralgia is primary, meaning there's no identifiable underlying cause. This is less common, but the pain still originates from the occipital nerves without obvious damage or compression from another condition. In such instances, the focus shifts to symptom management and nerve modulation.
Secondary Causes
Secondary occipital neuralgia arises from an underlying condition or injury that affects the occipital nerves. Common occipital neuralgia causes include:
-
Trauma: A head or neck injury, such as a whiplash injury from a car accident, can directly damage or compress the occipital nerves. This type of injury is a significant contributor, accounting for nearly 30% of diagnosed cases.
-
Inflammation: Conditions causing inflammation of the blood vessels (vasculitis) or tissues surrounding the nerves can lead to irritation.
-
Compression: Various factors can compress the nerves as they pass through muscles and tissues:
-
Tight Neck Muscles: Chronic muscle tension, particularly in the suboccipital muscles at the base of the skull, can entrap the nerves.
-
Osteoarthritis of the Upper Cervical Spine: Degenerative changes in the vertebrae of the neck can narrow the spaces through which the nerves pass.
-
Tumours or Cysts: Though rare, growths in the neck or at the base of the skull can press on the occipital nerves.
-
-
Degenerative Conditions: Conditions like cervical disc disease or cervical spondylosis can lead to nerve compression due to bone spurs or disc herniation in the upper neck.
-
Systemic Diseases: Diabetes, gout, and other systemic conditions can sometimes contribute to nerve damage, increasing susceptibility to conditions like occipital neuralgia.
-
Poor Posture: Prolonged periods of poor posture, especially common in office workers, can strain neck muscles and lead to nerve compression over time.
Recognising Occipital Neuralgia Symptoms
The symptoms of occipital neuralgia are quite distinct, making it possible to differentiate it from other types of headaches once a proper diagnosis is made. Recognising these occipital neuralgia symptoms is key to seeking timely medical attention.
Key Occipital Neuralgia Symptoms
-
Sharp, Shooting Pain: The hallmark symptom is sudden, piercing, or shock-like pain that originates at the base of the skull and radiates up towards the scalp, typically affecting one side but can be bilateral.
-
Burning or Throbbing Pain: In addition to sharp pain, individuals often describe a persistent aching, burning, or throbbing sensation in the affected area.
-
Tenderness of the Scalp: The scalp in the area supplied by the occipital nerves often becomes extremely sensitive to touch; even light brushing of hair can be painful.
-
Pain Behind the Eye: Many patients report pain radiating to the back of the eye on the affected side.
-
Sensitivity to Light (Photophobia): Some individuals experience increased sensitivity to light during episodes of pain.
-
Tingling and Numbness: These sensations may be present in the distribution of the affected nerve.
-
Pain Aggravated by Neck Movement: Turning or extending the neck can often trigger or worsen the pain.
It's important to note that while these symptoms are characteristic, they can sometimes overlap with other headache disorders, making an accurate diagnosis by an expert neurologist essential.
Diagnosing Occipital Neuralgia
An accurate diagnosis of occipital neuralgia relies on a comprehensive evaluation by a neurologist. This process helps rule out other conditions that might present with similar symptoms, ensuring the right occipital neuralgia treatment plan.
The Diagnostic Process:
-
Clinical Examination: Your neurologist will conduct a thorough physical examination, focusing on the head and neck. They will typically look for tenderness along the occipital nerves and may attempt to reproduce the pain by pressing on specific points at the back of your head.
-
Patient History: A detailed discussion of your symptoms, their onset, frequency, intensity, and any relieving or aggravating factors is crucial.
-
Nerve Blocks: A diagnostic nerve block, where a local anaesthetic is injected near the occipital nerve, is often the most definitive diagnostic tool. If the injection significantly relieves the pain, it strongly suggests occipital neuralgia. This method has a diagnostic accuracy rate of over 90%.
-
Imaging Studies: While X-rays, MRI scans, or CT scans do not directly show occipital neuralgia, they are often performed to rule out other structural causes of pain, such as tumours, spinal cord compression, or degenerative changes in the cervical spine.
Occipital Neuralgia Treatment Options
The goal of occipital neuralgia treatment is to alleviate pain, reduce inflammation, and address any underlying causes. Treatment approaches range from conservative therapies to advanced interventions, with a high success rate in pain reduction for many patients, often exceeding 70-80% with combined therapies.
Conservative Treatments for Occipital Neuralgia Relief
-
Heat and Cold Therapy: Applying heat packs to the neck and cold packs to the scalp can help reduce muscle tension and inflammation, offering temporary relief.
-
Massage and Physical Therapy: Specific massage techniques and physical therapy exercises can help release tight neck muscles, improve posture, and alleviate nerve compression. This can significantly reduce pain in up to 60% of patients.
-
Over-the-Counter Pain Relievers: Non-steroidal anti-inflammatory drugs (NSAIDs) can help manage mild to moderate pain and inflammation.
-
Prescription Medications: Your doctor may prescribe muscle relaxants to ease muscle spasms, anticonvulsants for nerve pain, or antidepressants that also have pain-relieving properties for more persistent symptoms.
-
Nerve Blocks: Therapeutic occipital nerve blocks, similar to diagnostic ones, involve injecting a local anaesthetic, sometimes combined with a corticosteroid, directly around the affected nerve. These can provide several weeks to months of occipital neuralgia relief and are effective for approximately 75% of patients.
-
Botulinum Toxin Injections: For chronic, refractory cases, injections of botulinum toxin into the muscles around the occipital nerves can help relax them, reducing compression and providing sustained pain relief for up to three months in about 65% of cases.
Advanced Interventions
For individuals who do not respond to conservative treatments, more advanced procedures may be considered:
-
Pulsed Radiofrequency Ablation (PRFA): This minimally invasive procedure uses radiofrequency energy to create a heat lesion on the nerve, temporarily blocking pain signals. It offers longer-lasting relief than nerve blocks for many patients.
-
Occipital Nerve Stimulation: An implantable device delivers mild electrical pulses to the occipital nerves, effectively masking pain signals. This is often considered when other treatments have failed, with patient satisfaction rates often exceeding 80%.
-
Nerve Decompression Surgery: In rare cases where an identifiable structure is compressing the nerve, surgical intervention to relieve pressure may be performed. This option is reserved for carefully selected patients and is highly effective when the cause is anatomical compression.
The choice of treatment will depend on the severity of your symptoms, the underlying cause, and your response to initial therapies. Our neurologists in Delhi work closely with patients to tailor the most effective treatment strategy.
Living with Occipital Neuralgia: Prevention and Management
While complete prevention of occipital neuralgia may not always be possible, especially if it stems from trauma or underlying medical conditions, several strategies can help reduce the risk of flare-ups and effectively manage the condition.
-
Ergonomic Adjustments: Optimise your workspace and home environment to support good posture. This includes proper chair height, monitor placement, and keyboard/mouse ergonomics.
-
Regular Exercise: Incorporate exercises that strengthen neck and core muscles, improving stability and reducing strain. Activities like swimming, yoga, and Pilates can be particularly beneficial.
-
Stress Reduction: Chronic stress contributes to muscle tension, which can trigger occipital nerve pain. Engage in hobbies, mindfulness, or professional counselling to manage stress levels.
-
Adequate Sleep: Prioritise quality sleep and ensure your sleeping posture supports your cervical spine.
-
Hydration and Nutrition: A balanced diet and sufficient hydration support overall nerve health and muscle function.
-
Early Intervention: If you experience persistent head or neck pain, consult a neurologist promptly. Early diagnosis and treatment can prevent the condition from becoming chronic and more difficult to manage. Many patients who seek early intervention experience a reduction in pain intensity by over 50% within weeks of starting treatment.
FAQ's
Occipital neuralgia can be triggered by various factors, including trauma to the head or neck, muscle tension in the neck, prolonged poor posture, compression of the occipital nerves by surrounding structures, and sometimes underlying medical conditions like osteoarthritis or tumours.
While not life-threatening, occipital neuralgia can be severely debilitating due to the intense and chronic pain it causes, significantly impacting a person's quality of life, ability to work, and daily activities. Early diagnosis and treatment are crucial to prevent long-term suffering.
For some, particularly when an underlying cause like muscle tension can be fully resolved, relief can be long-lasting or permanent. For others, especially in cases of nerve damage or chronic compression, management focuses on sustained pain relief and symptom control rather than a 'cure'. Many patients achieve significant, long-term relief through a combination of treatments.
Occipital neuralgia typically causes sharp, shooting, or electric shock-like pain originating at the base of the skull and radiating upwards, often on one side. Migraines are usually throbbing, widespread headaches often accompanied by auras, nausea, and extreme sensitivity to light and sound. While some symptoms can overlap, the character and location of the pain are key differentiators.
A neurologist is typically the specialist best equipped to diagnose and treat occipital neuralgia. They have expertise in nerve-related conditions and can offer a range of treatment options, from conservative management to advanced interventions. Pain management specialists also play a crucial role, often collaborating with neurologists.
Share this article on: