7 Min Read
7 Min Read
When you bump your knee or get a tiny scratch, your body immediately goes to work behind the scenes. Within minutes, a natural sealing process stops the minor bleeding, allows a small bruise to form, and begins the healing cycle without you having to give it a second thought. But for some individuals, this automatic internal repair crew lacks a vital tool, turning routine bumps into situations that require a bit more attention and care.
This blog breaks down exactly how this specialised bleeding variation operates within the body. You will discover the specific genetic factors behind it, how medical professionals classify its different severity levels, and the precise, modern therapies that allow individuals to manage their health effectively and live highly active lives.
Synopsis
- What is Haemophilia and How Does It Affect the Body?
- Types of Haemophilia
- Uncovering Haemophilia Causes and Genetic Links
- Common Bleeding Sites in Haemophilia
- Severity Levels and Daily Impact
- Emerging Role of Gene Therapy
- Living Safely with Haemophilia: Prevention and Daily Care
- First Aid During a Bleeding Episode
- Conclusion
What is Haemophilia and How Does It Affect the Body?
When someone asks what is hemophilia, they are looking at a rare, typically inherited condition that alters the blood's natural ability to form clots. The human body relies on a sequential process called the coagulation cascade to stop bleeding. When a blood vessel is damaged, platelets (tiny blood cells) rush to the site to form a plug, and specialised proteins called clotting factors act like biological glue to cement that plug firmly in place.
For individuals living with haemophilia disease, the body either produces an insufficient amount of a specific clotting factor or produces a version that does not function correctly. This means that if an injury occurs, the bleeding does not happen faster than usual, but it continues for a significantly longer duration because the structural glue cannot solidify. The two most common forms are Haemophilia A, where Factor VIII (eight) is deficient, and Haemophilia B, where Factor IX (nine) is missing.
Types of Haemophilia
Haemophilia is broadly classified into two major types depending on the clotting factor affected:
|
Type |
Clotting Factor Deficiency |
Incidence |
|
Haemophilia A |
Factor VIII (FVIII) |
1 in 5,000 male births |
|
Haemophilia B |
Factor IX (FIX) |
1 in 30,000 male births |
Haemophilia A accounts for nearly 80–85% of all diagnosed cases, while Haemophilia B constitutes approximately 15–20% of cases.
Uncovering Haemophilia Causes and Genetic Links
To understand haemophilia causes, we have to look closely at genetics, specifically the X and Y chromosomes that determine biological sex. The genetic instructions for producing vital clotting factors are located directly on the X chromosome. Biological males inherit one X chromosome from their mother and a Y chromosome from their father, so a mutation in that single X chromosome means their body cannot produce the factor properly.
Biological females inherit two X chromosomes. If one chromosome carries the mutation, the second working chromosome typically produces enough clotting factor to keep them healthy. While these females are considered genetic carriers and rarely experience severe symptoms, some can experience mild bleeding issues, such as heavy menstrual cycles. Interestingly, while the condition is mostly passed down through families, about one-third of all diagnosed cases occur spontaneously due to a sudden, unpredictable mutation in the gene during early fetal development.
While haemophilia is typically inherited, not every patient has a family history of the disorder. Approximately 30% of cases occur due to spontaneous genetic mutations. Interestingly, nearly half of children diagnosed with severe haemophilia have no known family history, making early recognition of symptoms especially important.
Recognizing Haemophilia Symptoms
The severity of haemophilia symptoms depends entirely on the baseline levels of clotting factors circulating in your blood. While individuals with a mild form of the condition might only experience prolonged bleeding after a major event like a surgical procedure or a tooth extraction, those with a severe form can experience bleeding episodes during everyday activities.
Key physical signs to monitor include:
-
Deep Tissue Bruising: Developing large, raised, or unexpectedly dark bruises from minor, everyday knocks that would not typically leave a mark on the skin.
-
Frequent or Unprovoked Nosebleeds: Experiencing heavy nosebleeds that start without any clear nasal trauma and take a considerable amount of time to subside using standard pressure.
-
Prolonged Bleeding from Minor Cuts: Noticing that a simple paper cut, a superficial scratch, or standard bleeding from the gums after routine dental brushing continues to ooze fluid for hours.
-
Internal Joint Bleeding (Haemarthrosis): This is one of the most defining and painful indicators of a severe clotting deficiency.
Common Bleeding Sites in Haemophilia
Bleeding episodes can occur in different parts of the body, with certain locations being more commonly affected:
|
Site |
Frequency |
|
Joints (knees, ankles, elbows) |
70–80% |
|
Muscles |
10–20% |
|
Gastrointestinal & urinary tract |
5–10% |
|
Brain (CNS) |
<5% |
Joint bleeding, particularly in the knees, ankles, and elbows, remains the hallmark feature of severe haemophilia and requires prompt medical attention to prevent long-term joint damage.
Severity Levels and Daily Impact
To determine the most effective management path, clinicians look at the exact percentage of clotting factors present in a person's bloodstream. The table below details how these structural differences change how the condition presents on a daily basis.
|
Severity Classification |
Factor Level in Blood |
Typical Clinical Manifestations |
|
Mild |
5% to 40% of normal baseline |
Bleeding usually occurs only after major physical trauma, surgical procedures, or tooth extractions. It might not be diagnosed until adulthood. |
|
Moderate |
1% to 5% of normal baseline |
Noticeable bleeding episodes can follow minor injuries, sprains, or deep bruises. Spontaneous bleeding without a clear cause happens occasionally. |
|
Severe |
Less than 1% of normal baseline |
Frequent spontaneous bleeding episodes occur, often directly into joints (knees, elbows, and ankles) or muscles without any known physical injury. |
The Diagnostic Pathway
Because a bleeding trend can point to several different circulatory variations, haematologists use a step-by-step laboratory screening process to establish an accurate haemophilia diagnosis. In haemophilia, a deficiency in clotting proteins prevents the mesh from forming properly. To pinpoint exactly where the clotting process is failing, medical teams use a series of targeted blood checks:
-
Complete Blood Count (CBC): This evaluates the overall volume and balance of your blood cells. It specifically checks your platelet count to confirm these primary plug-forming cells are working normally, ruling out a low platelet count as the source of your bleeding.
-
Activated Partial Thromboplastin Time (aPTT) Test: This measures the exact number of seconds it takes for a blood sample to form a visible clot. Because this test tracks the specific pathways where factors VIII and IX operate, an individual with haemophilia disease will show a significantly delayed clotting time.
-
Prothrombin Time (PT) Test: This test evaluates a separate pathway of the clotting process. It typically delivers a normal result in haemophilia patients, which helps specialists narrow down the diagnostic search.
-
Clotting Factor Assays: This is the definitive test used to confirm a diagnosis. It measures the precise percentage of factor activity inside the blood plasma, identifying whether the condition is Haemophilia A (missing Factor VIII) or Haemophilia B (missing Factor IX). It also scales the severity as mild, moderate, or severe.
Understanding Mixing Studies
When clotting tests show prolonged bleeding times, doctors may perform a mixing study. In this test, the patient's plasma is mixed with normal plasma.
· If clotting time normalizes, it suggests a clotting factor deficiency.
· If clotting remains prolonged, it may indicate the presence of inhibitors (antibodies) interfering with clot formation.
Mixing studies help differentiate classical haemophilia from acquired clotting disorders.
Modern Options for Haemophilia Treatment
Medical care has shifted away from simply reacting to injuries toward preventing complications before they even start. Today, haemophilia treatment options are structured around three main clinical approaches:
1. Factor Replacement Therapy
The baseline approach relies on infusing concentrated versions of the missing clotting factor directly into a vein to restock the body's natural supply.
-
Haemophilia A: Doctors prescribe specific recombinant Factor VIII concentrates, such as octocog alfa or the longer-acting efaloctocog alfa, which stays active in the bloodstream for an extended duration.
-
Haemophilia B: Treatment relies on Factor IX concentrates, such as nonacog alfa or the extended-life variant albutrepenonacog alfa.
These replacement infusions can be given on-demand to stop an active bleeding event quickly, or regularly at home as a preventative measure (prophylaxis) to maintain a constant, safe level of protection against hidden internal bleeds.
2. Advanced Non-Factor Therapies
For individuals managing Haemophilia A, newer therapies work without replacing the missing factor directly. A major option is emicizumab, a laboratory-engineered antibody that physically binds factors IX and X together. By doing so, it mimics the exact chemical action of the missing Factor VIII to restore the natural clotting pathway. Because it is given as a simple injection just under the skin (subcutaneously) once a week or once a month, it significantly reduces the need for regular vein infusions.
3. Supplemental and Localised Supports
For milder cases or specific medical procedures, doctors use localised treatments to support temporary clotting needs:
-
Desmopressin (DDAVP): Available as an injection or a specialised nasal spray for mild Haemophilia A. It stimulates the body's internal storage sites to temporarily release more of its natural reserves of Factor VIII into the circulation.
-
Tranexamic Acid: This antifibrinolytic medicine stops blood clots from breaking down prematurely. It is routinely prescribed alongside replacement factors to manage localised bleeding during dental procedures, minor oral injuries, or nosebleeds.
Emerging Role of Gene Therapy
Recent advances in gene therapy have transformed the treatment landscape for haemophilia.
Approved therapies include:
-
Roctavian (valoctocogene roxaparvovec) for severe Haemophilia A
-
Hemgenix (etranacogene dezaparvovec) for Haemophilia B
These one-time intravenous treatments deliver functional clotting factor genes to liver cells, enabling the body to produce clotting factors naturally. While not suitable for every patient, gene therapy represents a major step toward long-term disease control and reduced treatment burden.
Living Safely with Haemophilia: Prevention and Daily Care
Proper precautions can significantly reduce the risk of bleeding episodes and improve quality of life.
Safety Measures
-
Install safety gates around staircases for young children.
-
Avoid furniture with sharp edges.
-
Use helmets while cycling and travelling.
-
Wear knee and elbow guards during physical activities.
-
Prefer low-impact exercises such as swimming, walking, and cycling.
Vaccination Precautions
Vaccinations remain important for individuals with haemophilia. Whenever possible:
-
Use small-gauge needles.
-
Administer injections subcutaneously when appropriate.
-
Apply firm pressure at the injection site afterward.
Dental Health
Maintaining good oral hygiene helps reduce gum bleeding and minimizes the need for invasive dental procedures.
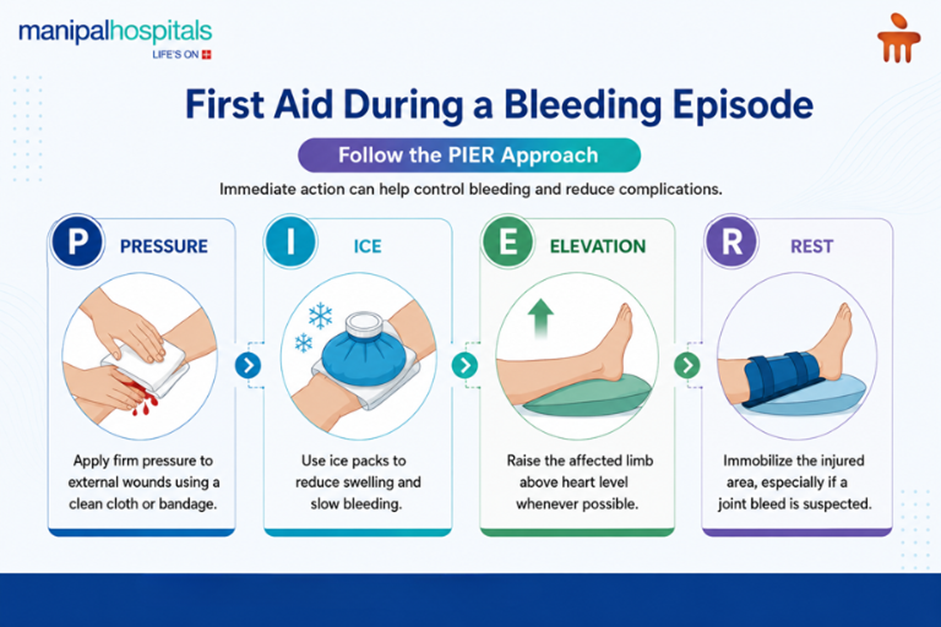
First Aid During a Bleeding Episode
Conclusion
Managing an inherited bleeding condition requires consistent monitoring and a reliable, preventative approach to care. If you require advanced factor tracking or want comprehensive haemophilia treatment in Varthur Road, Bangalore, booking a consultation at Manipal Hospitals, Varthur Road, Bangalore, connects you with advanced clinical support needed to manage your health safely and comfortably.
FAQ's
While the condition predominantly affects males due to its X-linked genetic nature, females can be impacted. A female can experience symptoms if she inherits the altered gene from both parents or if she is a carrier whose single active X chromosome does not produce a sufficient amount of clotting factor, leading to mild or moderate bleeding tendencies.
Yes, though it is exceptionally rare. This is known as acquired haemophilia. Unlike the inherited genetic form, it is an autoimmune condition where the body’s immune system mistakenly develops antibodies that target and destroy its clotting factors, typically Factor VIII. It is usually diagnosed in older adults or during late-stage pregnancy.
When bleeding occurs inside joint spaces, a condition called haemarthrosis, it causes swelling, warmth, and sharp pain, most commonly in the knees, elbows, and ankles. If these episodes happen repeatedly and you leave them untreated, the pooled blood damages the protective cartilage over time, leading to early arthritis and limited mobility.
High-impact contact sports like rugby, football, and boxing carry a high risk of head injuries and deep tissue bleeding, so they are generally discouraged. However, staying active is vital for joint strength. Low-impact activities such as swimming, cycling, and walking are highly recommended, especially when paired with a regular preventative treatment plan.
Diagnosis begins with screening tests, including an activated partial thromboplastin time (aPTT) test and a Prothrombin Time (PT) test, which measure how many seconds it takes for a blood sample to clot. If the aPTT test shows delayed clotting, a specific factor assay blood test is ordered to measure the exact percentage of Factor VIII or Factor IX present.
If you experience any signs of late postpartum haemorrhage symptoms, such as sudden heavy bleeding, large clots, dizziness, or fever, contact your doctor immediately or go to the nearest emergency room. Do not wait.
Share this article on: