6 Min Read
6 Min Read
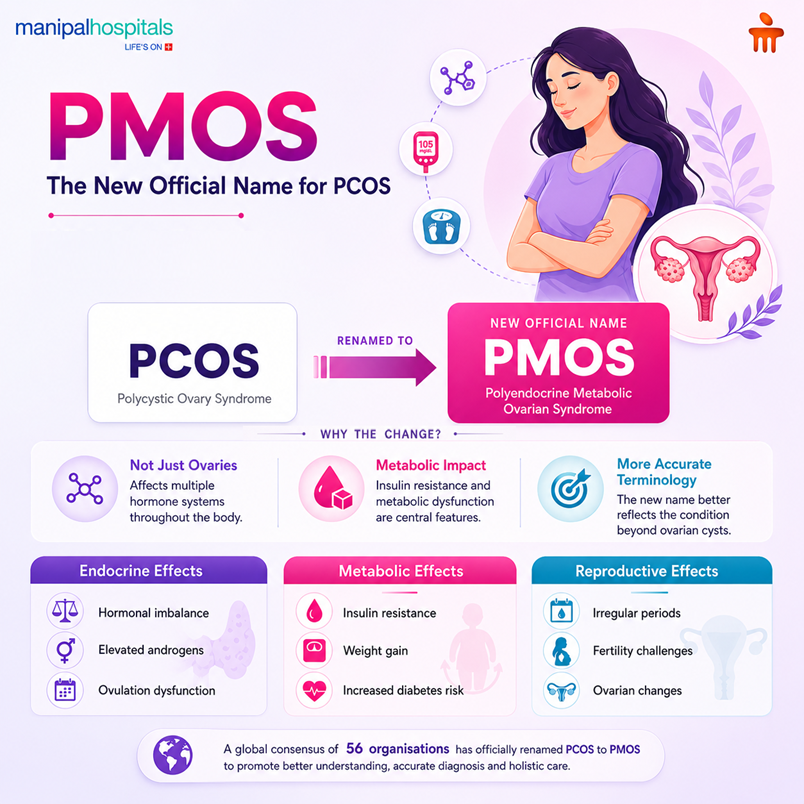
The global medical community is officially renaming Polycystic Ovary Syndrome (PCOS) to Polyendocrine Metabolic Ovarian Syndrome (PMOS) to reflect its full impact. The new name captures the reality that it involves multiple hormone systems, metabolic disturbances, and ovarian dysfunction from the start; it is not a progressive shift into a new disease.
When an underlying hormonal imbalance in women is left unmanaged for too long, the intertwined hormonal and metabolic disruptions can gradually lead to broader health concerns. Understanding how these systems interact is the most effective way to protect your health over the long haul. This blog explains how reproductive health and metabolism are tied together, how insulin resistance throws ovarian function off balance, and what steps help keep PMOS from driving long-term complications.
Synopsis
Understanding PMOS: The Core Concept
PCOS (Polycystic Ovary Syndrome) is focused on ovarian morphology, describing a condition where multiple small follicles (not true cysts) accumulate in the ovary, alongside hormonal imbalances and irregular ovulation. Because the term overemphasized "cysts," which are often absent, it was widely recognised as misleading.
Polycystic Ovarian Metabolic Syndrome accurately maps out the multi-system nature of the condition:
-
Polyendocrine: Multiple interlocking hormone pathways are altered, particularly involving elevated androgens (such as testosterone) and insulin.
-
Metabolic: It functions as a foundational metabolic disorder in women, frequently involving cellular insulin resistance, altered lipid profiles, and cardiovascular risks—even in individuals with a normal body weight.
-
Ovarian: The ovaries experience follicular development stalls and irregular ovulation, which can lead to PCOS and infertility challenges.
-
Syndrome: It is a collection of features that vary from person to person.
Irregular or absent ovulation makes conception more difficult, though many people with PMOS do conceive, sometimes with medical support. The change from PCOS to PMOS is a correction of the label, not a description of a new or worsened disease. While many clinicians, guidelines and medical records still use "PCOS"; the term PMOS more accurately represents the condition’s full-body nature.
How Does Insulin Resistance in PMOS Spark Hormonal Issues?
The key driver of ovarian hormonal dysregulation in PMOS is insulin resistance. A significant proportion of those with the condition, around 85%, have some degree of insulin resistance, even if body weight is normal. This metabolic feature is not a late complication but a core part of PMOS.
When cells become less responsive to insulin, the pancreas compensates by producing more of it. High circulating insulin directly stimulates the ovaries to increase androgen production and disrupts the normal maturation of follicles, contributing to anovulation and the appearance of multiple small follicles on ultrasound.
High insulin and androgen levels together encourage visceral fat accumulation. This abdominal fat is metabolically active and releases inflammatory substances that further impair insulin sensitivity. A self-reinforcing loop develops: metabolic imbalance worsens ovarian hormonal output, and the altered hormonal environment deepens the metabolic disturbance.
Key Symptoms and Indicators
As PMOS is a systemic endocrine disorder in women, symptoms manifest across several distinct physiological systems:Biological System
|
Biological System |
Clinical Symptoms |
Long-Term Health Risks |
|
Reproductive |
Irregular periods and PMOS-related cycle gaps, unusually heavy bleeding, and chronic anovulation. |
Endometrial thickening (hyperplasia) due to continuous estrogen exposure without balancing progesterone; elevated risks of PMOS and infertility. |
|
Metabolic |
Visceral weight gain around the abdomen, intense sugar cravings, and acanthosis nigricans (darkened, velvety skin patches around the neck or underarms). |
|
|
Dermatological |
Persistent adult cystic acne along the jawline, androgenic scalp hair thinning, and hirsutism (excess facial or body hair). |
Chronic skin inflammation, scarring, and psychological distress, including anxiety or low mood. |
How do doctors evaluate the condition?
Leading gynecology expert in Bhubaneshwar will be diagnosing PMOS to assess reproductive and metabolic health together. In adults, widely used criteria require at least two of the following, after excluding other causes:
-
Irregular or absent ovulation (indicated by menstrual cycle disturbance)
-
Clinical or biochemical signs of androgen excess
-
Polycystic ovarian morphology on ultrasound, or anti-Müllerian hormone (AMH) level as an alternative marker in adults
If irregular cycles and androgen excess are clearly present, imaging may not be necessary.
-
Hormonal Profiling: Blood tests measure total and free testosterone and often the ratio of Luteinising Hormone (LH) to Follicle-Stimulating Hormone (FSH). A raised LH: FSH ratio or elevated AMH supports the diagnosis. Thyroid function and prolactin are checked to rule out other causes.
-
Metabolic Screening: Fasting glucose alone can miss early insulin resistance. Evaluation typically includes fasting insulin, HbA1c, and sometimes an oral glucose tolerance test. A lipid panel assesses cardiovascular risk.
-
Pelvic Ultrasound: The scan looks for multiple small follicles (≥20 per ovary in adults) and measures endometrial thickness. A thickened lining in the absence of regular bleeding may indicate a need for cycle regulation to protect the endometrium.
In adolescents, diagnosis requires caution: irregular cycles can be normal soon after menarche, and ultrasound is generally not used for diagnosis in this age group.
Management and Lifestyle Strategies
Effective management targets both metabolic and reproductive aspects simultaneously.
-
Nutrition: A sustainable eating pattern built on high-fibre carbohydrates, lean protein, healthy fats, and limited highly processed foods and sugary drinks helps stabilise blood glucose and reduce insulin levels. There is no single “PMOS diet”; individualised guidance from a qualified dietitian can be valuable, especially when insulin resistance or weight concerns are present.
-
Physical Activity: Regular exercise enhances insulin sensitivity. Combining aerobic activity (such as brisk walking or cycling) with strength training improves glucose uptake by muscles and helps lower androgen levels. Even modest increases in daily movement are beneficial.
-
Medical Management: When lifestyle measures are insufficient, medication may be used. Metformin can improve insulin sensitivity and support metabolic and ovulatory function. Combined oral contraceptives or cyclic progestogens regulate menstrual cycles and protect the endometrium. Anti-androgen medications may be prescribed for significant hirsutism or acne, always with reliable contraception because of risks to a male foetus. For those trying to conceive, ovulation induction with letrozole is often the first-line treatment.
When to See a Doctor?
Early evaluation helps prevent long-term complications:
-
Routine consultation: Book an appointment if your periods are consistently irregular, infrequent, or absent for more than three months, or if you notice persistent acne, excessive hair growth, unexplained weight changes, or difficulty conceiving.
-
Urgent signs: Seek immediate medical attention for sudden severe pelvic pain, very heavy bleeding causing dizziness, or symptoms of high blood sugar such as excessive thirst, frequent urination, and unexplained fatigue. Rapidly worsening hirsutism or voice deepening also warrants prompt assessment.
Conclusion
Moving from the narrow “PCOS” label to the more accurate “PMOS” reflects a vital shift in how this condition is understood: it is a polyendocrine and metabolic disorder, not simply a reproductive one. Recognising the deep connection between hormonal balance and metabolic health changes the approach to care, steering it away from quick fixes and toward sustainable, whole-body wellness. Managing insulin resistance early helps protect fertility, metabolic function, and cardiovascular health.
For those seeking expert guidance, Book an appointment with top gynaecologists in Bhubaneshwar at Manipal Hospitals for PMOS treatment in the best Gynaecology hospital in Bhubaneswar ensures an accurate diagnostic evaluation and a structured, personalised care plan.
FAQ's
No. While PMOS is one of the most common underlying causes, hormonal imbalance in women can also result from thyroid disorders, elevated prolactin, adrenal conditions, high stress levels, or natural transitions such as perimenopause. A thorough medical evaluation is needed to identify the precise cause.
The two are closely linked through insulin resistance and androgen excess. When irregular periods and PMOS occur together, the underlying hormonal disturbance often involves high insulin and androgen levels that directly impair the body’s ability to regulate blood sugar, promote central adiposity, and raise the risk of type 2 diabetes and metabolic syndrome.
In many cases, yes. Consistent adoption of a balanced, lower-glycemic-load diet and regular physical activity can substantially lower circulating insulin, restore cellular insulin sensitivity, and reduce ovarian androgen production. This can significantly improve symptoms and metabolic markers, though some individuals may still require medication.
The connection centres on chronic anovulation. Because of the hormonal environment, the ovaries often fail to mature and release an egg each cycle. Without regular ovulation, conception becomes difficult. This lack of ovulation is the primary mechanism linking PMOS and infertility.
A general metabolic disorder, such as metabolic syndrome, may involve high blood pressure, dyslipidemia, and insulin resistance without directly affecting ovarian hormone function. PMOS (formerly PCOS) is a specific syndrome that combines these metabolic features with reproductive hormonal disruption, androgen excess, and ovulatory dysfunction, creating a distinct clinical entity that requires integrated gynecological and metabolic care.
Share this article on:











.webp "ଅଙ୍ଗ ଦାନର ଗୁରୁତ୍ୱ: ମୃତ୍ୟୁ ପରେ କେଉଁ ଅଙ୍ଗ ଦାନ କରାଯାଇପାରିବ?")