7 Min Read
7 Min Read
Have you been noticing belly pain after meals, bloating that won’t quit, or alternating constipation and diarrhoea? Those are the kinds of signs that make you ask whether this is just stress, something you ate, or irritable bowel syndrome (IBS). Although IBS isn’t life-threatening, it affects daily life and comfort, and knowing how to spot the pattern and manage it makes a big difference. Irritable bowel syndrome is a functional gut disorder where the gut doesn’t behave normally: there is pain, changes in bowel habits, and a range of other symptoms without a clear structural disease. This article describes common signs, likely causes, typical triggers, and practical approaches to care. It explains how screening and simple tests support an accurate IBS diagnosis, which in turn informs effective IBS management.
Synopsis
What is Meant by IBS?
Irritable bowel syndrome is a functional disorder of the gut that causes recurrent abdominal pain associated with changes in bowel habit. Clinicians use a symptom-based approach to make the diagnosis once alternative causes have been reasonably excluded. The condition is common and long-term but not life-threatening; appropriate IBS management helps many people restore normal activity and quality of life.
What are the Common IBS Symptoms?
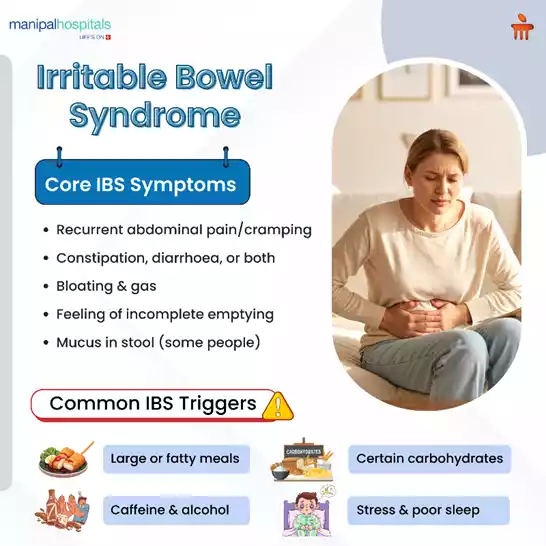
IBS symptoms are varied and can change over time. Typical features include:
-
Recurrent abdominal pain or cramps often improve after a bowel movement.
-
Changes in stool form and frequency, constipation, diarrhoea, or alternating patterns.
-
Bloating, gas, and a feeling of incomplete bowel emptying.
-
Mucus in the stool for some people.
-
Urgency or straining at the toilet.
You may see these IBS symptoms more during stress, after meals, or when routine changes occur. Specific foods or emotional stress often trigger IBS symptoms, so a clear pattern over weeks or months helps clinicians confirm the diagnosis.
IBS Symptoms in Females: What’s Different?
Women commonly report a slightly different symptom profile. IBS symptoms in females can include more abdominal pain before or during periods, more bloating, and higher rates of constipation-predominant IBS. Hormonal fluctuations and overlapping conditions like endometriosis or pelvic floor dysfunction can complicate the situation. For females, a careful history and targeted tests help rule out other causes and tailor management effectively.
What Causes IBS?
The exact causes of IBS remain complex and often multifactorial. Common contributing factors include:
-
Gut-brain axis changes: Communication between the gut and brain affects motility and sensitivity.
-
Altered gut motility: Bowels can move too fast or too slow.
-
Visceral hypersensitivity: The gut becomes more sensitive to normal stimuli, causing pain.
-
Post-infectious changes: Some people develop IBS after a stomach infection.
-
Gut microbiome imbalance: Changes in gut bacteria may play a role.
-
Psychological factors: Anxiety, depression, and chronic stress can worsen symptoms.
Understanding these IBS causes helps set realistic expectations: treatment aims to reduce symptoms and improve function rather than “cure” a single underlying cause.
Triggers and Foods to Avoid
Identifying IBS triggers is a practical step toward control. Common triggers include high-fat meals, large portions, caffeine, alcohol, and specific fermentable carbohydrates. The phrase "IBS symptoms foods to avoid" captures the idea that some items commonly provoke symptoms; these vary between people.
A staged approach works best: begin by logging diet and symptoms, then trial modest changes rather than broad exclusions. For many, a trial of the low FODMAP diet under dietetic supervision reduces bloating and IBS. This diet for IBS limits fermentable carbohydrates temporarily, then systematically reintroduces them to identify culprits. Avoiding foods based on guesswork can cause unnecessary restriction and nutritional gaps. Work with a dietitian when starting a diet for IBS to ensure it’s balanced.
How is IBS Diagnosed?
Diagnosis relies mainly on typical symptom patterns and ruling out other conditions. Key steps include:
-
Detailed history: frequency, relation to meals, stool patterns, and red flags (weight loss, bleeding).
-
Physical exam and basic blood tests to exclude inflammation or anemia.
-
Stool tests if infection is suspected.
-
Colonoscopy or imaging should only be considered if there are red flags or if symptoms begin after the age of 50.
The Rome diagnostic criteria are commonly used to define IBS; physicians use these criteria together with investigations to be confident in the diagnosis.
IBS Management: What Helps Reduce Symptoms?
IBS management combines lifestyle, diet, and sometimes medication. The approach is individualised, aiming to reduce symptom burden and improve quality of life.
Diet and lifestyle (first-line)
-
Fibre balance: Soluble fibre (like psyllium) can help constipation-predominant IBS; excess insoluble fibre may increase bloating.
-
Low-FODMAP diet: Short-term low-FODMAP restriction followed by gradual reintroduction helps identify triggers.
-
Regular meals and smaller portions.
-
Avoid excessive caffeine, alcohol, and fizzy drinks.
-
Hydration and physical activity to aid bowel regularity.
-
Stress management: Techniques such as mindfulness, CBT, or relaxation help reduce symptom flares.
Medications and therapies (when needed)
-
Antispasmodics are used to treat cramps and abdominal pain.
-
Laxatives for constipation-predominant cases and anti-diarrhoeals for diarrhoea-predominant IBS treatment.
-
Low-dose antidepressants for pain modulation in some patients.
-
Probiotics for IBS: Certain strains can improve bloating and stool pattern; results vary.
-
IBS management includes referral to gastroenterology or multidisciplinary teams for refractory or severe symptoms.
Quick Comparison of Common IBS Patterns
|
Feature |
Constipation-predominant (IBS-C) |
Diarrhoea-predominant (IBS-D) |
Mixed (IBS-M) |
|
Bowel habit |
Infrequent stools, hard or lumpy |
Loose or watery stools |
Alternates between hard and loose |
|
Main complaint |
Straining, incomplete evacuation |
Urgency, incontinence risk |
Unpredictable bowel pattern |
|
Helpful strategies |
Soluble fibre, laxatives, regular exercise |
Antidiarrhoeals, dietary triggers |
Tailored diet, stress management |
|
Pain pattern |
Cramping relieved by stool |
Cramping often with urgency |
Variable timing and severity |
When to Consult an Internal Medicine Specialist or Gastroenterologist?
See a doctor if you have:
-
Unexplained weight loss, persistent fever, or blood in stool.
-
New symptoms after age 50 or a family history of bowel disease or cancer.
-
Symptoms that don’t respond to initial lifestyle and dietary measures after several weeks.
-
Severe pain or significant disruption to daily life.
Gastroenterology Specialist help rule out conditions that mimic IBS and guide treatment, such as prescription medications, advanced testing, or referrals to dietitians and psychologists.
Meet Our Gastroenterology Experts at Manipal Hospital Salem
FAQ's
If symptoms follow the typical pattern of abdominal pain linked to bowel habits with no alarm features, clinicians consider a functional diagnosis. Tests exclude infection, inflammation, or anaemia; persistent red flags prompt further investigation.
No single list fits everyone. Many find benefit by trialling the low FODMAP diet guided by a dietitian to identify personal triggers rather than adopting blanket restrictions.
Yes. Stress and anxiety commonly amplify gut sensitivity and motility, so addressing psychological factors is a valid part of IBS management.
Women may note symptom variation with menstrual cycles and a higher frequency of constipation or bloating. Recognising these patterns supports personalised care.
If first-line medicines and diet do not control symptoms, referral to a specialist clinic can explore alternative options, psychological therapy, or advanced testing to refine treatment.
Share this article on: